Digital Dry Eye
Introduction
The digital environment is ubiquitous in modern life (Figure 1). A global prevalence of digital eye strain has been estimated to affect on average 70.7% of an adult population (Wolffsohn et al., 2023), but ranged widely from 31.9% in bank workers in Italy (Mocci et al., 2001) to 97.3% in university students in Saudi Arabia (Altalhi et al., 2020). The Tear Film & Ocular Surface Society (TFOS) Workshop (www.tearfilm.org), entitled ‘A Lifestyle Epidemic: Ocular Surface Disease,’ establish the direct and indirect impacts that everyday lifestyle choices and challenges have on ocular surface health (Craig et al., 2023).
- The digital environment (of relevance to eyes) is defined as any technology requiring viewing of a digital display for a cognitive task.
The potential effect(s) of digital device use on vision and eye health have been studied for over 20 years (Dain et al., 1988), highlighted by several recent literature reviews (Mehra and Galor, 2020, Sheppard and Wolffsohn, 2018, Coles-Brennan et al., 2019, Gowrisankaran and Sheedy, 2015, Kamøy et al., 2022). The most commonly quoted definition is from the American Optometric Association that states “Computer vision syndrome, also referred to as digital eye strain, describes a group of eye- and vision-related problems that result from prolonged computer, tablet, e-reader and cell phone use” (American Academy of Optometry, Accessed March 2022). However, this definition does not exclude those who experience these ‘problems’ when conducting similar non-digital tasks and key terms such as “prolonged” are not defined. Hence the TFOS Lifestyle Workshop Digital Environment report (Wolffsohn et al., 2023), defined the term:
- Digital eye strain as “the development or exacerbation of recurrent ocular symptoms and/or signs related specifically to digital device screen viewing”.
The term ‘digital eye strain’ was used in preference to ‘computer vision syndrome’ as ‘computer’ technology can be considered quite specific and ‘vision” is less appropriate terminology than ‘strain’ meaning to “over-exert” (2022) relating to the ‘eye’. Other past terminology includes: ‘repetitive strain disorder’ (Munshi et al., 2017), eye fatigue (Meyer et al., 2021), ‘eye related pain’ (Thorud et al., 2012), ‘asthenopia’ (Chu et al., 2014, Meyer et al., 2021) and even ‘video game vision’ has been proposed (Mylona et al., 2020).
Management and Advice
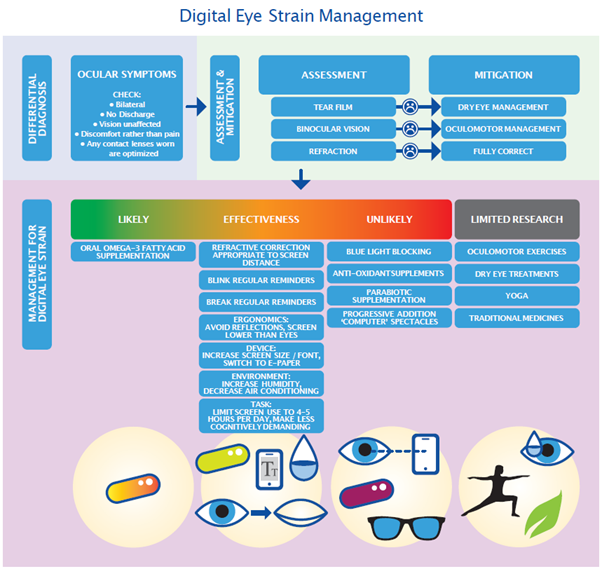
Although many studies have been conducted to evaluate treatments for digital eye strain, the quality of these studies is variable (Wolffsohn et al., 2023). The intervention with the strongest evidence of a benefit to individuals with digital eye strain is:
- Oral omega-3 fatty acid supplements.
Well researched treatments which have been found to have no beneficial effect in ameliorating digital eye strain are blue light blocking and anti-oxidants. Other strategies where there is some evidence that they may be affective include:
- Optimising the refractive correction for the screen distance
- Regular blink and break reminders
- Placing the screen lower than the user’s eyes and avoiding reflections
- Increasing the screen size / font and potentially switching to e-paper
- Increasing the humidity and decreasing air-conditioning in the users environment
- Limiting screen use to under 4-5 hours a day and / or reducing the cognitive demand of the task(s)
Areas which warrant further research include:
- Oculomotor exercises
- Dry eye treatments
- Yoga
- Traditional medicines
Prognosis
It is unknown whether untreated digital eye strain can lead to increased symptoms of eye health problems in the future. However, as well as ocular, visual and musculoskeletal symptoms, the presence of digital eye strain has been associated with lower quality of life (Hayes et al., 2007) and reduced work productivity (Daum et al., 2004). Hence, trying to minimise digital eye strain is warranted.
Prevention: Optimising the ocular surface / tear film, binocular vision and refraction of all patients should minimise the chances of them experiencing digital eye strain when circumstances require extended period of digital device use.