CLAPC/ Contact lens associated Papillary Conjunctivitis
Patient presentation
Patient had come in twice already prior to seeing me for the first time, the reason for visit being the same as the previous two times. Patient’s complaints/RFV was irritable sensation after taking lenses out itchy, scratchy, sore eyes, vision doesn’t feel the same with contact lenses /reduced vision doesn’t feel as comfortable. These symptoms were also recorded in the previous two visits and no improvement since patient said but little better on the vision side.
On the first visit the patient’s prescription was changed, on the second visit patients contact lens was changed to a different monthly lens.
On the visit with me I probed further on the History and symptoms, patient was a excess 7/7 monthly contact lens user with a 10 year CL history, foreign body feeling in eye that became worse when taking lenses and also these symptoms became more apparent with no CL inserted.
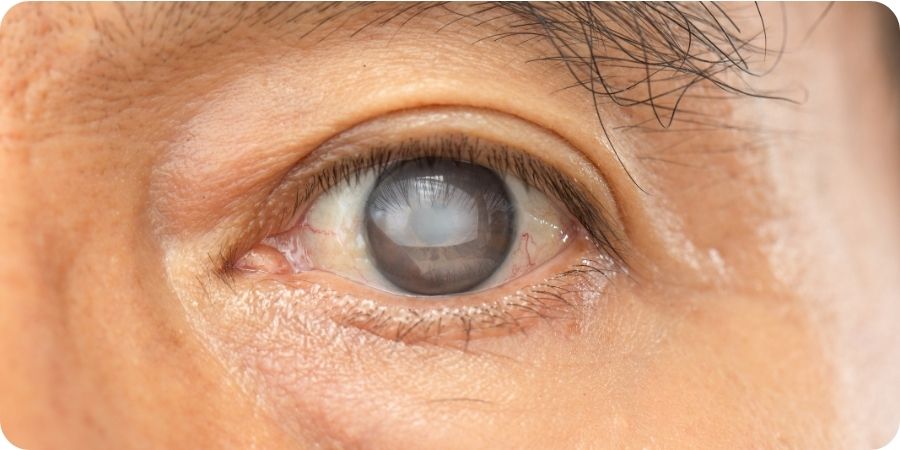
Unfortunately, no evidence of lid eversion was done in the first two visits confirmed by asking patient as well, it was clear it was CLAPC in both eyes when lids were everted lower lids papillae was fine but upper lids grade 2-3 (Efron scale/ES) both eyes. Now I wouldn’t class it as GPC as the papillae was not enlarged more than 1mm, but all papillae were roughly 0.5-1mm.
In this video, which is not the same patient as my case, can estimate that some papillae here in this video are 1mm or greater but the patient I managed I only saw 1-2 papillae was about 1mm and rest were smaller. I’m not sure if this indicated I caught it early.
Diagnosis and Management
This patient always sticks out mainly because I’ve managed this patient for one of the longest periods of time until I had to refer as I was not seeing any results I would’ve liked, and also because I did this whilst I was nearly finished my pre-registration scheme so was unable to find slots with myself as consistently as I would’ve liked. The management was prolonged more than I would’ve preferred, and it took a while until I referred for the patient to be seen.
I initially changed the patient to Acuvue 2-weekly lenses from Biofinity monthly (this is what was given on the second visit) & changed the solution to peroxide solution from multipurpose, dropped wear time to max 10-12 hours and 5 days a week.
Px also had Blepharitis grade 2 (ES) both eyes no collarettes noted so did also advise lid hygiene with lid wipes. I told the patient to take oral antihistamine daily.
After 8 weeks I saw the patient again and I saw no improvement at all in the CLPAC but the blepharitis had improved to grade 0.5(ES) both eyes
I changed the patient to daily contact lenses as patients’ motivation for using contact lenses had started to drop and Px felt ‘not happy in them anymore’. I told the Px to cease contact lenses for 4 weeks to continue with the oral antihistamine whilst also using sodium cromoglicate as instructed on NHS website for 4 weeks then discard the bottle. I also advised cold compress once a day 5-10min a day and rebooked for a follow up in 5 weeks time.
Patient was unable to make the appointment and I left a voice message to continue with everything but not the sodium cromoglicate and only use contact lenses when required and rely on glasses and come in the earliest slot available which was now in total 7 weeks.
On examination, nearly 4 months since I’ve first seen the Px. Patient does feel happier and says appreciates the follow ups, service and management care given and I trust the patient in following the therapy guidelines. Does feel improvement to vision and comfort. Does not feel like its totally gone. Findings showed a reduction in CLAPC from grade 2-3 to grade 2 (ES) so it hadn’t improved to as much as I would’ve liked. The size of the papillae also remained the same.
I advised preservative free dry eye drops (Hycosan Dual) which also has ectoin to help with allergy response in eye, patient to use this daily until bottle finishes 3x a day (in hindsight I could’ve given these drops to Px on the visit when I was also treating the blepharitis). Currently at this stage of patient management I felt like I was trying to chuck everything in my arsenal at the patient hoping one thing works. I thought there had been some improvement and time would be a factor in the road to recovery, so I advised the patient to continue with previous advice of cold compress, antihistamine orally still, rely on glasses as much as possible and the Hycosan dual drops.
I rebooked patient to come back in 1 month, as I was not in work as regularly to prepare for my OSCE, I left clinical advice just to refer patient if no change to CLAPC. Patient was unable to make the appointment with myself and refused to be seen by anyone else so waited a further 1 month to be seen by me.
It has now been in total 23 weeks patient has been in my care and additional 3.5 weeks since patient first came in with these complaints. This is now more than half a year patient has been putting up with this; this may be relevant for the findings of the visit.
On this visit patient says its no longer a problem anymore I feel fine I don’t have anymore of those symptoms and my vision feels fine I wear the CL 5days a week and12 hours max. On examination I did not see any difference to previous visit so I referred patient routinely for management as it has not resolved on clinical findings. I found it odd that patient had said they no longer feel anymore symptoms but I think it may because they are using drops and oral antihistamines.
I didn’t see this patient for another 9 months until they were received a routine reminder. Px had received NSAID drop treatment. On examination can see it resolved to where patient just had junctional papillae grade 1 (ES) where it was also much more smaller papillae 0.1-0.15mm. The patient continues to use Hycosan Dual drops and has ceased using cold compress, lid hygiene wipes and oral antihistamine. Patient is still closely monitored for blepharitis, CLPAC, GPC alongside other common CL related eye disease on Aftercare appointments.
Conclusion
If I was IP qualified, I would’ve managed the CLPAC quicker and patient wouldn’t have to wait as long to be treated. I think this would benefit the patient with being able to use contact lenses more and more trust in clinical care as this must’ve felt long process to recovery for patient. Patient costs also as had to pay for various different therapy for some not even complete resolution.
Latest Articles



HCP Popup
Are you a healthcare or eye care professional?
The information contained on this website is provided exclusively for healthcare and eye care professionals and is not intended for patients.
Click ‘Yes’ below to confirm that you are a healthcare professional and agree to the terms of use.
If you select ‘No’, you will be redirected to scopeeyecare.com
This will close in 0 seconds