Post-Cataract Surgery Dry Eye Disease
Post-cataract surgery dry eye disease is one of the most commonly overlooked challenges in modern eye care. Despite affecting up to 80% of patients undergoing cataract surgery, ocular surface disease remains underdiagnosed, under documented, and undermanaged, particularly at the critical interface between primary and secondary care.
This article, developed from the OSI Dry Eye Master Class & Symposium 2026, is written specifically for optometrists who sit at the front line of both pre and post-operative care. It covers the pre-operative risk stratification, DEWS III Frameworks, Shared care considerations and some practical patient cases studies.
The Scale Of The Problem
The data highlights just how significant this issue is in everyday practice:
- In England alone, there are approximately 400,000 cataract procedures performed each year within the NHS . That translates to a very large number of patients at risk of developing or worsening dry eye symptoms.
- Importantly, dry eye is the number one cause of dissatisfaction after successful cataract surgery. Symptoms typically persist for three to six months, although recovery can take longer in certain groups such as patients with diabetes or previous refractive surgery .
- The key message is simple. Most cataract patients either already have ocular surface disease or will develop it during their surgical journey.
Why does this matter for optometrists?
- First in Line: Most patients attend community optometry for their first post-op eye test, you are first to identify problems.
- Accurate Refraction: Unrecognised DED → unstable tear film → fluctuating vision → inaccurate refraction → wrong glasses → dissatisfied patient.
- Surgical Planning: Pre-existing DED documented in referral letters can change surgical planning and IOL selection.
Evidence Base: TFOS DEWS Reports
Three landmark reports define our current understanding of dry eye disease and its relationship to cataract surgery.
Defined DED. Established diagnostic methodology, severity grading, and treatment stepladder. Still the primary clinical reference for grading systems used today.
Formally codified surgery, including cataract surgery, as an iatrogenic cause of DED. Pre-operative ocular surface optimisation became a recognised clinical standard.
Updated definition (launched Nov 2023, published 2025). Revised diagnostic methodology, updated management algorithms, and incorporated iatrogenic dry eye as a distinct topic.
DEWS III: Updated Definition (2025)
“Dry eye is a multifactorial, symptomatic disease characterized by a loss of homeostasis of the tear film and/or ocular surface, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities are etiological factors.”
Always Symptomatic
Both signs AND symptoms required for diagnosis. Ocular surface signs alone = ‘ocular surface disease’, not DED.
Newly Screened with OSDI-6
6-item questionnaire, cut-off ≥4. Simpler than the original 12-item OSDI for clinical screening.
Iatrogenic DED Formalised
Surgery (including cataract) explicitly recognised as a cause. Pre-op optimisation is now an evidence-based standard.
Pathophysiology: Four Surgical Mechanisms
Cataract surgery disrupts the ocular surface through four distinct mechanisms, all converging on tear film instability and the perpetuation of a vicious inflammatory cycle.
Incisional Nerve Damage
Sub-basal plexus transection produces a neurotrophic effect, reducing corneal sensation and blunting the patient’s perception of dry eye symptoms.
Perioperative Eyedrops
Povidone iodine, NSAIDs, and BAC preservative toxicity from perioperative drops directly damage the epithelial surface and sustain post-operative inflammation.
Phototoxicity
Microscope light causes photochemical damage to the corneal epithelium and conjunctival goblet cells, reducing mucin production and tear film stability.
Surgical Trauma
Speculum use, irrigation, phacoemulsification energy, and FLACS suction rings all contribute to ocular surface disruption and goblet cell loss.
Tear film instability → hyperosmolarity → inflammation → goblet cell loss → reduction in mucin → further instability. BAK-preserved drops sustain the cycle post-operatively. Nerve recovery takes 3–6 months (longer in diabetes and post-LASIK). Surgery unmasks or worsens pre-existing MGD.
Pre-Operative Risk Stratification
High-Risk Patient Profile
- Previous LASIK / refractive surgery
- Pre-existing DED of any severity
- Sjögren’s syndrome or autoimmune disease
- Diabetes mellitus (subclinical neurotrophic keratopathy)
- Post-menopausal female
- Rosacea / established MGD
- Prolonged contact lens wear
- Systemic medications: antihistamines, antidepressants, isotretinoin
Pre-Op Optometry Checklist
- OSDI-6 questionnaire (≥4 = positive screen)
- NIBUT target >10s; <5s = abnormal
- Fluorescein corneal staining: Oxford grade
- Lissamine green: conjunctival + lid wiper
- Meibomian gland expression: grade meibum 0–3
- Lid margin: telangiectasia, anterior blepharitis
- Document objective scores in referral letter
- Flag premium IOL requests: surface must be stable
Clinical Signs: What to Look For
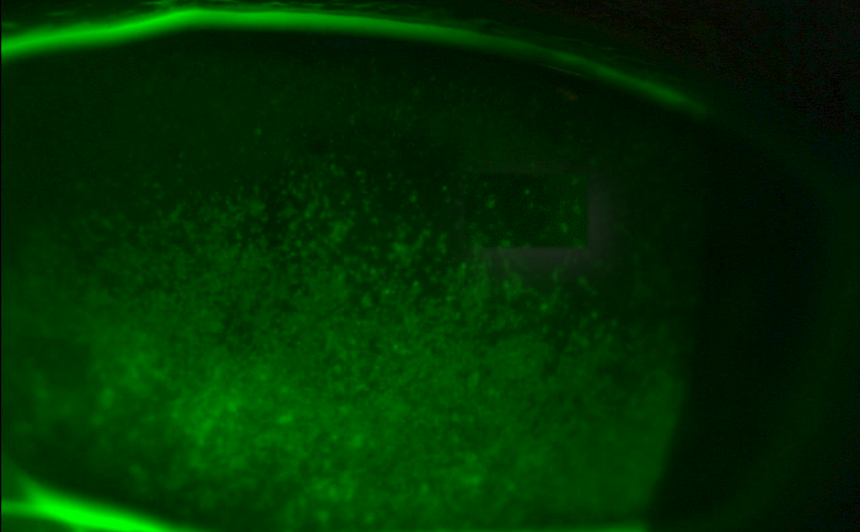
Corneal Staining: Oxford Grade
Fluorescein + cobalt blue. Grade I–IV. Post-cataract: typically inferior distribution. Grade ≥II warrants treatment.
Conjunctival Staining
Lissamine green. Nasal + temporal conjunctiva and lid wiper zone (upper lid, everted). Apply before fluorescein.
NIBUT
Non-invasive break-up time <10s = abnormal. <5s = significantly abnormal. The single most useful objective test in community practice.
Meibum Quality
Grade 0 (clear) → Grade 3 (toothpaste). Express lower lid glands at slit lamp. MGD grade drives treatment choice.
DEWS III Driver-Based Treatment Framework
DEWS III principle: Identify the etiological driver(s), then select matched evidence-based therapies. Most patients have overlapping drivers so combine treatments accordingly.
- PF artificial tears (sodium hyaluronate, Thealoz Duo, AEON, Hylo Tears)
- Lid hygiene with warm compresses and lid wipes
- Omega-3 / nutritional supplementation
- Environmental modification, blink optimisation
- Lipid-containing drops (e.g. Hycosan Shield / PFHO)
- In-office lid warming: IPL, LipiFlow, Blephasteam
- Punctal plugs (after inflammation addressed)
- Tear stimulation: nasal neurostimulation
- Autologous serum / PRP (severe – refer)
- Blinking exercises, blink awareness training
- Screen break hygiene
- Lid hygiene: Blephasol, Blephaclean wipes
- Topical antibiotic/steroid if active inflammation
- Demodex: lotilaner 0.25% (Xdemvy: not yet UK) or tea tree oil products
- Warm compresses + manual expression
- IPL (first line for rosacea/telangiectasia)
- Low-level light therapy
- Vitamin D3 supplementation
- Doxycycline 50mg OD (rosacea/severe MGD)
- Ciclosporin 0.1% (Ikervis) – NICE TA369
- Short-course topical steroid (loteprednol / dexamethasone PF)
- Serum tears – autologous or allogeneic (NHSBT)
- Cenegermin (Oxervate) – neurotrophic keratitis, NHSE IFR
- Scleral contact lenses
- Amniotic membrane (Prokera – NHS specialist)
- Punctal cautery
- Tarsorrhaphy (severe exposure/lagophthalmos)
Shared Care: Who Does What?
Community Optometry: Manage
- Mild–moderate DED (Oxford I–II, OSDI-6 <15)
- Initiate Steps 1 and 2
- Monitor and re-grade at 6–8 weeks
- IPL for MGD (if trained and equipped)
- Punctal plug insertion
- Monitor ciclosporin (Ikervis) response
- Pre-op ocular surface optimisation
- Patient education and counselling
Refer Back to Ophthalmology
- Oxford ≥III not responding to Step 2
- OSDI-6 ≥15 persisting at 3 months
- Filamentary keratitis
- Reduced corneal sensation + PED (neurotrophic)
- Corneal ulceration or stromal thinning
- Sjögren’s with severe aqueous deficiency
- Autologous serum or scleral lens potentially needed
- Diagnostic uncertainty
Referral letter ideally includes: OSDI score · Oxford grade · NIBUT · meibum grade · treatments tried + duration
Workshop Cases
Three illustrative cases from clinical practice, demonstrating recognition, management, and escalation of post-cataract dry eye disease.
History
- Bilateral LASIK 14 years ago (mentioned in passing)
- No dry eye symptoms, feels completely well
- OSDI-6 score: 2 (below screening threshold)
- Otherwise fit, no systemic conditions
- Graphic designer with significant screen time
- Requesting premium EDOF/toric IOL
Examination Findings
- Corneal topography: irregular mire pattern, map distortion RE
- NIBUT: 6s (RE), 7s (LE)
- Lissamine green: moderate nasal & temporal conjunctival staining
- Lid wiper epitheliopathy: upper lids bilaterally
- Meibum quality: grade 2 (granular, upper and lower lids)
- Schirmer’s: 14mm (aqueous production normal)
Diagnosis: Ocular surface disease (pre-symptomatic LASIK-reduced corneal sensation). MGD grade 2. Irregular topography from tear film instability. High-risk for severe post-cataract DED.
Pre-Op Actions
- PF HA 0.2% QDS: start immediately, before referral
- Warm compresses BD + lid hygiene
- Omega-3 supplementation
- Consider IPL referral for MGD (4 sessions)
- Repeat topography after 6 weeks of treatment
- Refer once topography has stabilised
Referral Letter Must Include
- Bilateral LASIK 14 years ago: HIGH RISK FLAG
- Objective findings: NIBUT 6s, lissamine staining, LWE, MGD grade 2
- OSDI-6 = 2 but OSD present with symptom-sign dissociation
- Topography irregular; biometry reliability reduced
- EDOF not advisable until surface stable; toric: reassess after optimisation
- Treatment initiated: state drugs, dose, start date
History
- ‘The lens must be wrong, my vision is blurry’
- Vision fluctuates throughout the day, worse in evenings
- OSDI-6: 9 (moderate range)
- Maxitrol QDS since discharge (still using)
- PMHx: T2DM 10 years (HbA1c 58), post-menopausal
- No previous dry eye history documented
Examination Findings
- VA: 6/12 unaided, 6/9.5 with pinhole (marginal improvement)
- Refraction: +0.25DS (minimal change from unaided)
- NIBUT: 4 seconds
- Fluorescein: Oxford grade III, inferior corneal distribution
- Meibum: grade 2, mild lid margin telangiectasia
- IOL position normal; no PCO at 5 weeks; normal OCT macula
Diagnosis: Post-cataract evaporative DED, moderate (DEWS II grade 2). NIBUT 4s, Oxford III, OSDI-6 9. VA reduction from tear film optical irregularity (not an IOL or refractive problem). Compounded by BAC-preserved Maxitrol and diabetes.
Immediate Actions
- Contact surgical team: switch Maxitrol to PF dexamethasone (Minims Dexamethasone PF)
- PF HA 0.2% (Hylo-Forte) minimum QDS, not PRN
- Warm compresses BD + lid hygiene (Blephagel)
- Omega-3 supplementation
- Explain clearly: blurry vision = tear film instability, not the IOL
- DO NOT prescribe glasses today
- Review in 6–8 weeks: re-OSDI, re-stain, then refract
If Not Improved at 6 Weeks
- Upgrade to viscous PF HA + carbomer gel nocte
- If Oxford still ≥II at 3 months: refer back and consider ciclosporin initiation
- Note: DM slows nerve recovery to allow longer timeline before escalating to Step 3
- Refraction more reliable when NIBUT >7s and staining has reduced
History
- 6-week surgical review: ‘mild dry eye, uses drops (Systane Ultra)’
- Constant foreign body sensation and photophobia
- OSDI-6: 14 (severe range)
- Systane Ultra QDS: no improvement
- PMHx: Sjögren’s syndrome (quiescent, on hydroxychloroquine)
- Rheumatology unaware of surgery; surgical team unaware of Sjögren’s
Examination Findings
- VA: 6/18 LE; pinhole 6/12 (limited improvement)
- NIBUT: <3 seconds
- Corneal staining: Oxford grade IV, inferior and central
- Schirmer’s: 2mm/5min – severe aqueous deficiency
- Filamentary keratitis: mucus filaments visible on inferior cornea
- Corneal sensation: reduced compared with fellow eye
Diagnosis: Severe aqueous-deficient DED, Sjögren’s syndrome decompensated by surgery. Filamentary keratitis. Oxford grade IV. Schirmer’s 2mm. URGENT same-week ophthalmology referral required.
Immediate Actions (Your Chair)
- STOP Systane Ultra and switch to PF HA (Hylo-Forte PF) every 1–2 hours
- Add PF carbomer gel nocte (Viscotears PF)
- Telephone surgical team today: same-week review
- Referral letter: OSDI 14, Schirmer 2mm, Oxford IV, filamentary keratitis, reduced corneal sensation, Sjögren’s
- Notify GP/rheumatology: surgical stress may have triggered systemic flare
What Ophthalmology Will Likely Do
- Filament debridement ± N-acetylcysteine 5%
- Autologous serum 20% (NHSBT referral)
- Topical PF steroid
- Ciclosporin 0.1% (Ikervis) initiated
- Lower punctal plug insertion / punctal cautery
- Oxervate (cenegermin) if neurotrophic keratitis confirmed
- Scleral contact lens assessment if not resolving
Five Key Take-Aways
- Up to 80% of cataract patients have pre-existing OSD: common, often subclinical, frequently absent from the referral letter.
- DEWS III 2025: DED is always symptomatic. Both signs AND symptoms required. OSDI-6 (≥4) is the new recommended screening tool.
- Pre-op assessment changes surgical outcome. LASIK history, Sjögren’s, MGD grade and topography belong in every cataract referral letter.
- Stepwise management works. PF lubricants, lid hygiene, steroid ± ciclosporin. Most cases are community-manageable. Know your referral triggers.
- Objective numbers drive appropriate triage. OSDI score, Oxford grade, NIBUT in the referral letter.
References
- Gupta P, Drinkwater O, VanDusen KW et al. Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation. J Cataract Refract Surg 2018;44:1090–1096.
- Trattler WB, Majmudar PA, Donnenfeld ED et al. The PHACO study: the effect of dry eye. Clin Ophthalmol 2017;11:1423–1430.
- NHS England. Getting It Right First Time (GIRFT) Ophthalmology National Specialty Report. London: NHS England; 2021.
- Epitropoulos AT, Matossian C, Berdy GJ et al. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg 2015;41:1670–1677.
- Cho YK, Kim MS. Dry eye after cataract surgery and associated intraoperative risk factors. Korean J Ophthalmol 2009;23:65–73.
- Wolffsohn JS, Benítez-Del-Castillo JM, Loya-Garcia D et al. TFOS DEWS III: Diagnostic Methodology. Am J Ophthalmol 2025;279:387–450.
- Jones L, Craig JP, Markoulli M et al. TFOS DEWS III: Management and Therapy. Am J Ophthalmol 2025;279:289–386.
- Stapleton F, Argueso P, Azar D et al. TFOS DEWS III: Digest. Am J Ophthalmol 2025;279:451–553.
- Craig JP, Nelson JD, Azar DT et al. TFOS DEWS II: Definition and Classification. Ocul Surf 2017;15:276–283.
- Wolffsohn JS, Arita R, Chalmers R et al. TFOS DEWS II: Diagnostic Methodology. Ocul Surf 2017;15:539–574.
- Craig JP, Jones L, Diaper C et al. TFOS Lifestyle Report: Iatrogenic Dry Eye. Ocul Surf 2023;28:304–309.
- Starr CE, Gupta PK, Farid M et al. ASCRS Cornea Clinical Committee: Pre-op OSD algorithm. J Cataract Refract Surg 2019;45:1243–1288.
- NICE Technology Appraisal TA369. Ciclosporin (Ikervis) for severe dry eye disease. NICE; 2015.
- Baudouin C, Aragona P, Messmer EM et al. Role of hyperosmolarity in the pathogenesis and management of DED. Prog Retin Eye Res 2016;55:47–75.
- Wolffsohn JS, Trave-Huarte S, Craig JP et al. OSDI-6 thresholds for diagnosis and monitoring of dry eye disease. J Clin Med 2024;13(11):3146.

Latest Articles



HCP Popup
Are you a healthcare or eye care professional?
The information contained on this website is provided exclusively for healthcare and eye care professionals and is not intended for patients.
Click ‘Yes’ below to confirm that you are a healthcare professional and agree to the terms of use.
If you select ‘No’, you will be redirected to scopeeyecare.com
This will close in 0 seconds