Optimising the Ocular Surface Before Refractive Surgery
The American Refractive Surgery Council has estimated that approximately 30% of patients experience short-term dry eye following LASIK. Furthermore, 21% of patients seeking a second opinion after LASIK do so because of dry eye-related concerns. The good news is that with proper pre-operative evaluation and treatment, the huge majority of our patients can avoid these issues. It may delay treatment in some cases, but in a modern refractive surgery practice where our patients’ outcomes are prioritised, it is essential to respect the ocular surface.
Despite this data, pre-operative dry eye assessment is too often treated as a box to be ticked rather than a clinical priority that shapes the entire surgical plan.
“The ocular surface is the transparent foundation upon which all clear vision is built. If the foundation is unstable, nothing built on it will last.”
What Pre-operative Assessments should we do ?
A robust pre-operative dry eye assessment begins before the patient sits at the slit lamp. Structured, validated questionnaires provide an objective baseline and establish a shared language between clinician and patient for describing symptoms.
1. OSDI and SPEED Questionnaires
The Ocular Surface Disease Index (OSDI) and the Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire are both widely used and well-validated tools for quantifying dry eye symptom burden. These should be administered routinely as part of the pre-operative workup — not as a formality, but as a scored clinical measure that will inform management decisions. The OSDI6 questionnaire can be downloaded here
2. Full Patient Case History
The questionnaire alone is insufficient. A thorough clinical history should specifically explore the following symptom domains:
- Fluctuating or variable vision throughout the day
- Morning blurriness on waking
- Symptoms related to prolonged screen use
- Glare sensitivity or halos
- Burning sensation
- Gritty or foreign body sensation
Critically, these findings must be documented formally and — just as importantly — communicated verbally to the patient. Naming dry eye as the likely cause of pre-operative visual fluctuations, fatigue, and discomfort sets accurate expectations and significantly reduces the risk of post-operative dissatisfaction. If a patient is experiencing fluctuating vision before surgery, they need to understand why — and that optimising the tear film is a prerequisite for a successful outcome.
Objective tests
Clinical history and validated questionnaires provide the subjective dimension of the assessment. Objective diagnostic tests are then required to characterise the tear film and ocular surface with precision. Four core investigations should be performed as standard.
3. Tear Osmolarity
Two-thirds of refraction occurs at the air-tear film interface.
With normal tear osmolarity, there is a stable tear film resulting in high and stable ocular image quality. With abnormal tear osmolarity, there is tear film instability and fluctuating ocular image quality that impacts visual performance
Tear osmolarity is a direct biomarker of tear film homeostasis and is one of the most informative objective tests available. In healthy subjects, osmolarity remains remarkably stable across the day — typically below 300 mOsm/L — with minimal diurnal variation or inter-eye difference.
In patients with dry eye disease, this stability breaks down. Elevated osmolarity and increased inter-measurement variability are hallmarks of the condition (Keech, Curr Eye Res, 2013). The downstream consequences are significant: hyperosmolarity disrupts the corneal glycocalyx and microvilli — the structures responsible for retaining the aqueous layer on the corneal surface. This disruption leads to tear film instability, progressive surface damage, and ultimately epithelial cell death. The result is the clinical staining pattern commonly observed on fluorescein or lissamine green examination.

4. Non-invasive Tear Break-up Time (NITBUT)
Non-invasive tear break-up time quantifies lipid layer function and tear film stability without the confounding effect of fluorescein instillation. A NITBUT of less than 7 seconds is a clinically significant finding that influences both patient selection and procedural choice. Patients with a borderline NITBUT may tolerate certain refractive procedures poorly, and this measurement should therefore be reviewed alongside osmolarity data when making decisions about candidacy and technique.

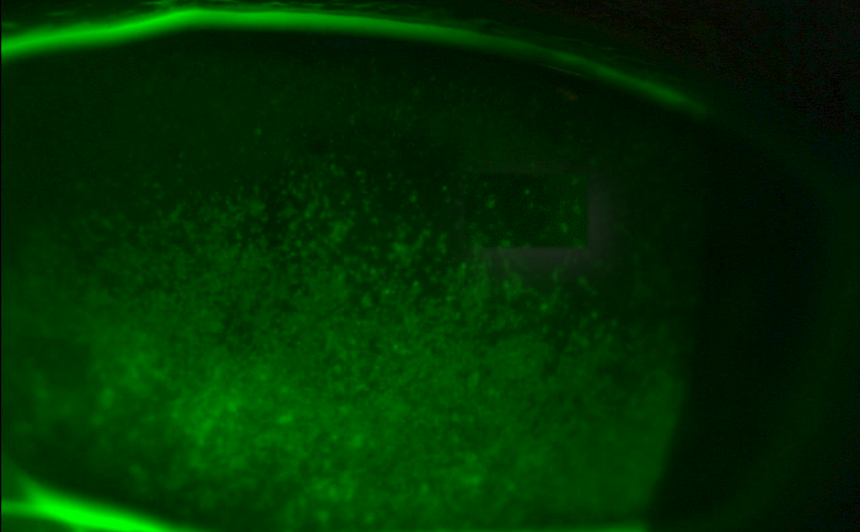
5. Corneal Staining
Fluorescein and lissamine green staining provide direct evidence of ocular surface compromise. Staining patterns — whether punctate, diffuse, or in characteristic locations — reflect the cumulative damage from tear film hyperosmolarity and instability. The presence and extent of staining should be graded and documented, as it represents one of the most visible indicators of current ocular surface health and forms part of the composite assessment when timing surgical intervention.

6. Meibography and Meibomian Gland Expression
Assess the number and status of meibomian glands. Meibomian gland dysfunction (MGD) is the most common underlying cause of evaporative dry eye and is prevalent across refractive surgery populations, including many patients who are not yet symptomatic. Meibography — typically performed using infrared imaging — allows direct visualisation of gland morphology, revealing atrophy, truncation, or dropout that may not be apparent from clinical history alone.
Meibomian gland expression assesses the quality and quantity of secretion and provides functional information that complements the structural data from meibography. Together, these investigations determine whether MGD is a contributing factor and whether targeted treatment — such as heat therapy, gland expression, or more advanced interventions — will be required as part of the pre-operative optimisation programme.

How Does Dry Eye Affect Planning of Interventions? Part 1 — Accuracy of Procedure
Every refractive surgery pathway — whether laser vision correction, lens replacement surgery, or lens addition surgery — depends on a comprehensive suite of pre-operative measurements. For laser procedures, this includes manifest and cycloplegic refraction, keratometry, Pentacam tomography, topography, epithelial mapping, and biometry where relevant. For lens-based procedures, additional measurements such as corneal astigmatism assessment, vision quality metrics, endothelial cell counts, and ultrasound biomicroscopy may also be required.

The critical point is this: all of these measurements assume a stable, healthy tear film. When the ocular surface is compromised, measurement accuracy is degraded — often in ways that are not immediately obvious.
The Effect of Hyperosmolarity on Keratometry and IOL Calculations
Research has demonstrated that hyperosmolar eyes show significantly greater variation in corneal astigmatism (Kcyl) measurements between clinical visits compared to eyes with normal osmolarity. In one study, 17% of hyperosmolar eyes showed more than 1 dioptre of change in Kcyl values between two visits, compared with a single eye in the normoosmolar group — a statistically significant difference (p=0.013). This degree of variability would directly translate into error in IOL power calculations for cataract and lens replacement surgery.
“The principle is simple and should be embedded in every pre-operative protocol: optimise the ocular surface before diagnostics. No surprises.”
Advanced technology IOL’s –
- Depend on excellent optics, including optimised tearfilm
- Need accurate biometry and topography to determine the optimal IOL power
- Need an excellent ocular surface to enjoy the benefits of the AT-IOL: Dry eye amplifies photic phenomena
How Does Dry Eye Affect Planning of Interventions? Part 2 — Choice of Procedure ?
LASIK and the Dry Eye Threshold
Following LASIK, most patients experience a temporary increase in ocular surface sensitivity lasting approximately 3 to 6 months. In a patient with excellent pre-operative tear function, this transient reduction is easily navigated — the tear film recovers without significant symptomatic impact. However, in patients who are already borderline, or who have subclinical dry eye that has not yet produced symptoms, the same post-operative reduction can push them across the symptom threshold.
The clinical consequence is a patient who attributes their dry eye symptoms entirely to the surgery — when in fact the surgery has simply unmasked a pre-existing condition. This distinction is difficult to explain convincingly after the fact and represents one of the most common sources of post-LASIK dissatisfaction.
When to Consider ICL or Lens Replacement
For patients with established, symptomatic dry eye, implantable collamer lens (ICL) surgery or lens replacement are generally preferable to LVC. ICL surgery preserves corneal nerve integrity and does not carry the same risk of exacerbating tear film dysfunction. Published comparative data supports this — postoperative dry eye rates are significantly lower following ICL than following femtosecond LASIK, with differences persisting at 12 months post-operatively.
How Do We Optimise the Ocular Surface Before Surgery?
When dry eye or meibomian gland dysfunction is identified pre-operatively, the appropriate response is not to defer surgery indefinitely — it is to treat, reassess, and proceed only when the ocular surface is ready. A structured pre-operative optimisation protocol protects both the patient and the clinical outcome.
Addressing Meibomian Gland Dysfunction
Where MGD is present, it should be treated directly. The core interventions include:
- Warm compress therapy, ideally using a moist heat mask to achieve consistent lid margin temperature
- Meibomian gland expression to physically clear obstructed glands and restore lipid layer function
- Regular preservation free hyaluronic acid eye drops appropriate to the patient’s specific tear film deficiency
Lifestyle Modifications
Non-pharmacological measures can meaningfully improve tear film quality and should form part of any optimisation programme:
- Reducing prolonged screen use and implementing structured blinking exercises
- Dietary modification, particularly reduction in refined sugar intake
- Omega-3 fatty acid supplementation, which has an evidence base for improving meibomian gland secretion quality
- Smoking cessation
Advanced Treatments
Where standard measures are insufficient, or where the degree of MGD or ocular surface inflammation warrants a more targeted approach, the following options should be considered:
- Intense Pulsed Light (IPL) therapy — particularly effective for MGD with associated dermatological features such as rosacea
- Low Level Light Therapy (LLLT)
- Topical cyclosporine — for cases with a significant inflammatory component
The key principle of pre-operative optimisation is sequencing: treat first, then measure. Diagnostic data obtained before the ocular surface is stable will not reliably represent the eye that will be operated on. Building this protocol into the routine clinical workflow protects outcomes and professional reputation alike.
“The goals of refractive surgery can be distilled to three outcomes: excellent vision, maximum safety, and no unhappy patients. Dry eye threatens all three.”
A patient who achieves 6/6 but experiences fluctuation or dryness is not a satisfied patient. Preventing that outcome begins well before surgery: with patient education, thorough ocular surface assessment, and a willingness to do the preparatory work that premium outcomes demand — including, when necessary, the clinical confidence to recommend not operating at all. Optimise the surface first, operate on stable data, and patients will have their best vision from day one.

Latest Articles


HCP Popup
Are you a healthcare or eye care professional?
The information contained on this website is provided exclusively for healthcare and eye care professionals and is not intended for patients.
Click ‘Yes’ below to confirm that you are a healthcare professional and agree to the terms of use.
If you select ‘No’, you will be redirected to scopeeyecare.com
This will close in 0 seconds