Introduction
Over the last decade there has been a increased incidence of anterior segment eye surgeries being performed across both the public and private sector. Anterior segment surgeries include procedures such as; cataract surgery, corneal transplantation, microinvasive glaucoma surgery (MIGS) and laser refractive surgery.
The exact number of cataract surgeries globally can vary significantly due to differences in healthcare systems, access to care, and reporting practices. Estimates suggest that cataract extraction is performed approximately; 3.7 million cases per year in the USA; 7 million cases per year in Europe and 20 million cases per year worldwide1. Demand for cataract surgery is expected to continue growing in the coming years2,3 due to an aging population and increased life expectancy. In addition, advances in technology and surgical techniques may improve outcomes and increase the attractiveness of both lens based and laser refractive surgeries.
Common invasive anterior segment procedures include:
Corneal surgery
- Lenticule Extraction e.g. SMILE
- LASIK
- Keratoplasty (DMEK/DSEK/DALK/PKP)
Cataract Surgery
- Clear Lens Extraction (CLE)
There is clear evidence that dry eye disease (DED) can be exacerbated by these procedures4,5, and this can result in ongoing patient discomfort and dissatisfaction with the procedure. Because of this there are a number of patients whose quality of life (QOL) is adversely affected to a significant degree.
While most of the research and technological advancements in eye care focus on improving outcomes and preventing serious vision problems, it is important not to forget about the less severe side effects, even though they’re not sight threatening.
The impact of DED goes beyond the patients’ post-operative experience. It’s also a key factor in a clinic achieving accuracy in cataract and refractive surgery. Accurate topography, tonometry, and biometric measurements are essential for surgical planning and great post-op vision6,7. It is well acknowledged that a healthy, intact pre-corneal tear film8 is required as it is the eye’s first refractive component. Therefore, to maximise accuracy a complete pre-op assessment for surgery should also include a comprehensive screen for DED.
There are a few steps listed below that take place as part of the surgical pathway that will cause or exacerbate existing dry eye. These steps are necessary e.g. using antiseptic eyedrops pre-op to reduce the risk of infection, but the clinical team should be aware of the potential impact on the ocular surface.
- Repeated drying/irrigationDuring cataract surgery, the eye’s surface is exposed and goes through cycles of drying and irrigation to keep things clear for the surgery. This can potentially harm the corneal and conjunctival surfaces.9, 10 The use of an ophthalmic visco-surgical device (OVD) during the procedure coats the ocular surface and has been shown to significantly improve TBUT, OSDI scores and ocular surface staining 1 week post-operatively.11
- Intra operative drops
– Iodine/Povidone
– Anaesthetics
– Non-steroidal anti-inflammatory drops (NSAIDS)
– Preservatives in eye drops e.g. benzalkonium chloride (BAK)Ocular surface damage may be due to the toxic effects of eye drops. The use of eye drops during and after surgery may lead to potentially harmful effects on the ocular surface with injury to corneal epithelial and conjunctival epithelial and goblet cells.12
Using povidone-iodine just before surgery is excellent for reducing the risk of post-operative endophthalmitis,13 but studies have shown it can be toxic to the corneal surface14, 15 The same goes for topical anaesthetic drops which can cause similar issues.16, 17 So, it’s important to carefully choose the type and amount of these drops, especially for patients with existing dry eye or other eye surface diseases. After routine cataract surgery, patients usually get a mix of steroid, anti-inflammatory, and antibiotic drops as part of their care. These drops often have preservatives, which studies have found can be harmful to the ocular surface. 18, 19
- Photo toxicity form lamps and microscope
Studies have shown that the light from the operating microscope can have phototoxic effects on the eye’s surface.20-22 It’s still unclear how much this phototoxicity, along with factors like the drying of the eye during surgery and the need for frequent irrigation, contribute to dry eye disease (DED) after cataract surgery. This needs more research, with a focus on each factor individually. In the meantime, for patients at risk of DED after cataract surgery, it’s a good idea to limit the exposure to the operating light as much as possible to avoid eye surface damage and potential DED-related issues.
- Surgical Trauma
– Speculum
– Opening Femtosecond Laser (FL) Incisions
– Femtosecond Laser-assisted Cataract surgery (FLACS) Suction Ring
Corneal nerve damage can occur intra operatively in surgery such as LASIK, PRK and cataract surgery. This can affect the radial stromal nerves, particularly in full thickness wounds in cataract surgery. The result of this can lead to a disruption of tear film homeostasis.23
Over the years various studies have shown that cornel nerve function is reduced post cataract surgery and may still be reduced up to 3 months after the operation.24 Patients are warned of this loss of sensation pre-operatively along with the potential exacerbation of DED that may result after the procedure. Surgical trauma can also arise from the use of the speculum intra operatively, femtosecond laser (FL) incisions, and femtosecond laser assisted cataract surgery (FLACS) suction rings may lead to ocular surface damage which can include the corneal epithelium and the conjunctival epithelial goblet cells as well as corneal nerves as already mentioned
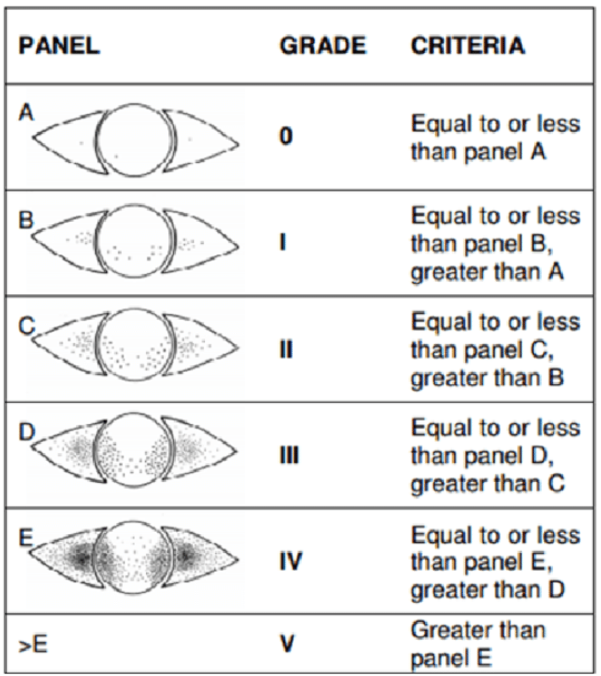
The incidence of dry eye post cataract surgery varies widely in the literature and ranges from 9% to 100% in different studies depending on clinical markers.12 Ishrat et al. reported clinical signs of DED in 9% of patients 4 weeks after surgery.5 On the other hand, Miyake and Yokoi documented such problems in 31% of patients at the same time period.25 Interestingly in a prospective study of 100 patients, Dasgupta and Gupta found that at 12 weeks post-surgery, 100% of patients had a tear break up time (TBUT) abnormality.16 Helpful diagnostic and treatment algorithms, such as the ASCRS Preoperative OSD Algorithm27 have been proposed to help identify pre-existing dry eye and management algorithm to maximise refractive accuracy and patient comfort through the surgical journey.