Locked in and unresponsive to botox
Patient Presentation
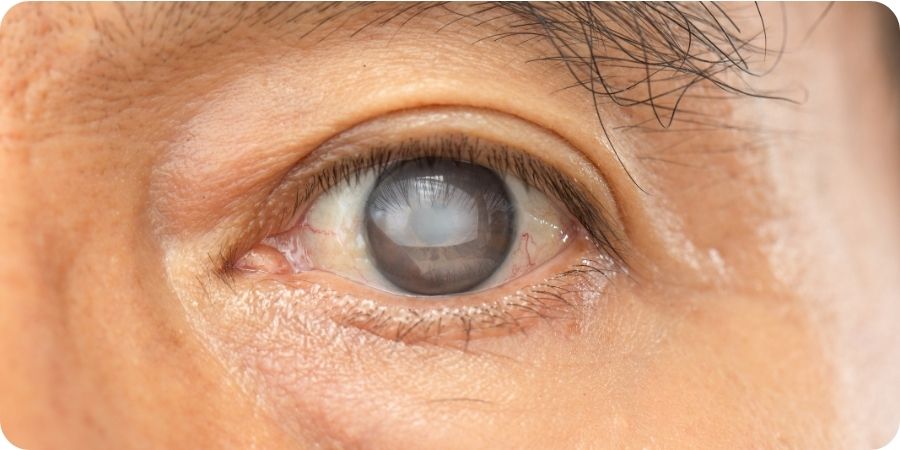
We present a case of a 33 year old Caucasian woman who was an inpatient on an acute rehabilitation ward. She had suffered a significant cerebrovascular accident during complications during childbirth and was diagnosed with Locked-in syndrome. She had otherwise been previously fit and well with no previous ocular history. Despite quadriplegia, she maintained her blink reflex and cognitive function and was able to communicate minimally through this. The Ophthalmology team was called as the patient had developed a red right eye despite attempted taping at night and regular use of ointment. On examination her upper eyelids appeared retracted more so on the right, there was a poor blink reflex and it was difficult to encourage the patient to close her eyes. Using portable equipment she was also noted to have marked hyperaemia of her conjunctiva, and there was a corneal central linear epithelial defect with some infiltrate. There was no hypopyon. Her left eye anterior segment examination was normal. Due to difficulties in communication, her symptoms and visual acuity could not be determined but she was on occasion fixing and following our movements.
Diagnosis and management:
She was started on topical antibiotics to treat her microbial keratitis and as she was already on lubricant ointment four times a day it was decided to administer botox to her upper eyelid to drop the eyelid and improve protection. Consent was provided by her relatives as a best interest decision. 40 units of Xeomin R (botulinum toxin A) was administered through the anterior approach. She was reviewed a few days later, and was found to have no change in her eyelid position. Her cornea appeared only slightly improved. It was presumed the previous botox injection had not been enough or administered inadequately to affect the levator and so a further 60 units was injected posteriorly, through the conjunctiva surface of the superior tarsal edge. She was again reviewed a few days later and it was noted that her right upper eyelid had only improved by a few millimetres and was now in a position just at the limbus. Instead of proceeding with a more invasive tarsorrhaphy it was decided to create a moisture chamber, using: Jelonet R, ocular preservative free ointment Hylo Night R and an eye shield. This seemed to accelerate her improvement. Eventually her cornea was clear and she was back to the her lubricant ointment Hylo Night R only. During this entire follow up period of a few weeks her injected upper eyelid never dropped further than the limbus.
Conclusion:
Botox is commonly used for a number of reasons, including inducing ptosis where there is a need to protect the ocular surface. It acts by binding to the pre synaptic neurones that use acetylcholine to transmit signals. It is taken up by the axon and in turn prevents the release of the neurotransmitter acetylcholine, thus disabling signals through these neurones. Most commonly botox fails when it is not administered in the right place, the dose is too small, or when repeated use results in resistance. Given the botox in our case was injected through two methods directly targeting the levator and high doses were used in a treatment naïve patient, it was unique that this patient should respond so minimally to treatment. Locked-in syndrome is a complex and rare medical condition, with the classical form defined by complete immobility, with the preservation of the ability to perform vertical eye movements, blink and maintain a normal levels of consciousness. Often there is damage to various structures such as the pons, mesencephalon and thalamus. Establishing communication is a main goal of rehabilitation. One report suggests that eyelid retraction can be a feature of locked-in syndrome and can be caused by damage to the third nerve fascicle and the nucleus of the posterior commissure. The later sends inhibitory fibres to the central caudal nucleus and damage can result in disinhibition of the levator palpebrae. We postulate that the botox did not work in this case as the cause of the eyelid retraction is central and is a disinhibition whilst botox often targets more peripheral neurones.
We feel this case exemplifies the challenges involved when treating complex patients, compounded by difficulties in communication, and the fine line between ensuring optimal care whilst balancing this with the extent of invasiveness when acting in their best interests. It shows that even in these challenging situations and when the unexpected occurs, there are still various options to consider for treatment.
Latest Articles



HCP Popup
Are you a healthcare or eye care professional?
The information contained on this website is provided exclusively for healthcare and eye care professionals and is not intended for patients.
Click ‘Yes’ below to confirm that you are a healthcare professional and agree to the terms of use.
If you select ‘No’, you will be redirected to scopeeyecare.com
This will close in 0 seconds