Bilateral pigment dispersion glaucoma
Patient presentation
- Eye examination date 26th April 2024
- New patient. Female, aged 58 years
- Myopic both eyes
- The patient was recommended by her family Optometrist in the Republic of Ireland to visit me because of poor vision in new spectacles.
- Last eye examination February 2024
- Advised cataracts at last sight test Feb 2024
- History of dry eyes and blepharitis – well controlled
- General health good – suspect hyperglycaemia, under investigation with GP
- No family history of eye disease including glaucoma
- No flashes or floaters
- No reported headaches or diplopia
- Occupations: Driver, Office worker, art galleries, running and swimming
Diagnosis and Management
VAs in current spectacles R +0.32 L +0.34
Cover test Orthophoric in existing glasses at distance and near
Todays refraction and VAs:
R-5.50/+0.25×180 VA +0.30
L-7.00/+0.25×180 VA +0.34
Add +2.00 N6 both eyes
Pupils normal – PERRLA
Tonometry
Pulsair IOPs at 12.25pm R 22 L 29 mmHg
Goldmann IOPs at 12.30 R 23 L 30 mmHg
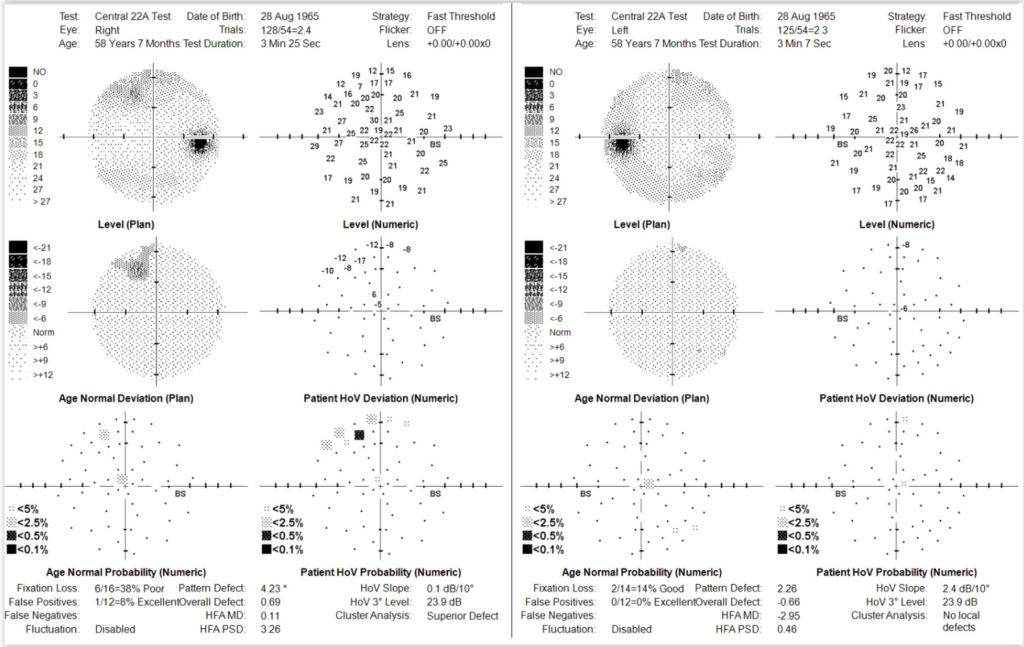
Visual fields (Medmont Central 22A thresholded fields)
Right superior ring defect (artefact, and poor reliability)
Left eye normal – no local defects (good reliability)
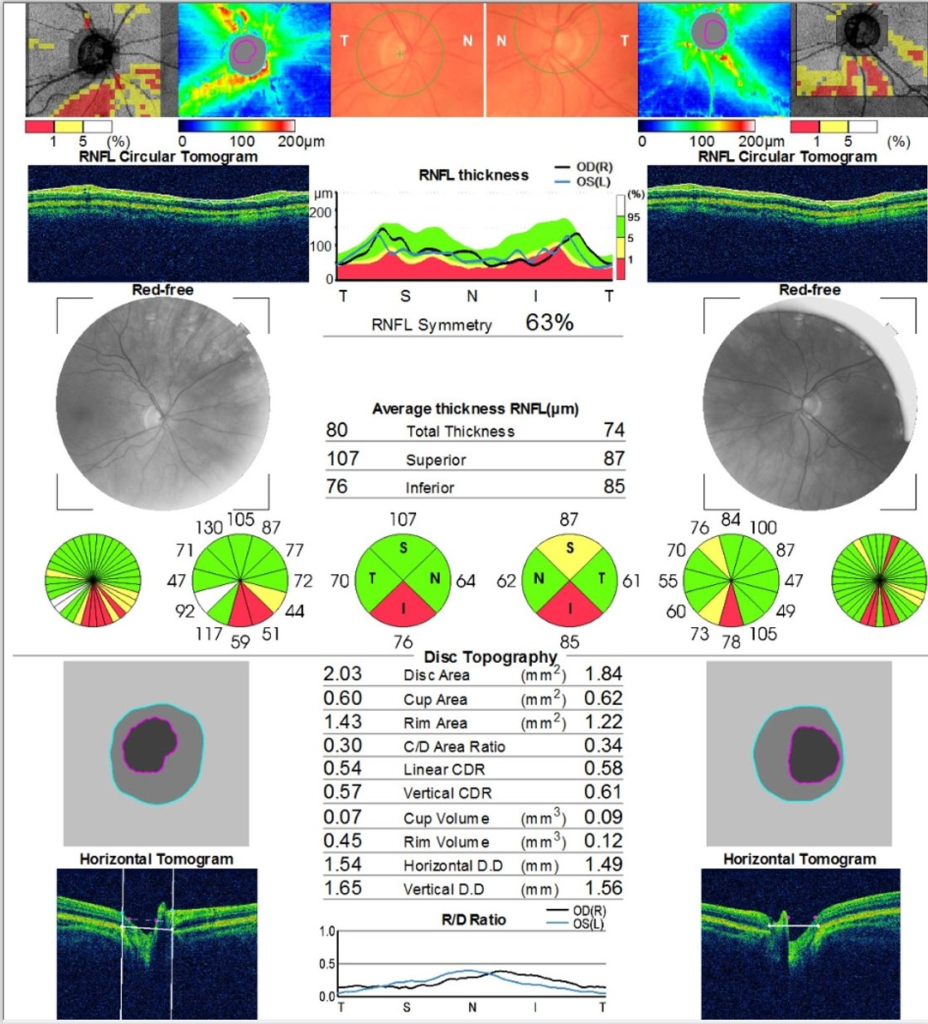
Topcon Maestro OCT
Maculae – normal profile and bright reflexes
Central Corneal thickness scan R552 L 534 microns
Optic Discs – RNFL asymmetry seen. Both eyes show inferior RNFL thinning. Relatively large cups for the smaller than average size of the optic nerves
Slit lamp examination – anterior segment
Anterior blepharitis grade 2 both eyes
Anterior segment – anterior chamber wide grade 4 Van Herricks both eyes
Posterior segment and slit lamp BIO with 0.5% tropicamide both eyes:
Bilateral moderate cortical cataracts
Vessels – normal crossings and no arteriosclerosis or hypertensive changes seen
Maculae – Bright reflexes
Fundus and periphery – Flat pink and healthy with no lesions tears holes or detachments
Optic discs:
Right CD 0.4 Inferior pallor of NRR with well defined margins
Left CD 0.6 Inferior pallor of NRR with well defined margins
Discussed bilateral cataract and an inability to improve visual acuity using new spectacles. Patient was offered referral for cataract extraction and wished to go ahead. Discussed with patient that there was evidence of open angle glaucoma in the left eye (raised IOP) and possibly even some evidence of optic nerve damage in the right eye too despite normal IOPs
I suggested that we have the eye pressure and suspect glaucoma checked by a glaucoma consultant, as well as having the cataracts evaluated for surgery by the same consultant. Since cataract surgery would impact on eye pressure I thought it prudent to discuss seeing a glaucoma consultant before cataract extraction, since the surgery options may potentially be altered to reduce eye pressure if appropriate (such as using iStents).
The patient was offered an NHS hospital referral with a wait of approximately 6 months to be seen, alternatively to see a local glaucoma specialist privately within the next few weeks
Patient chose the private option to expedite treatment. A referral was sent to the private clinic via email and the patient was seen 2 weeks later.
Conclusion
The patient was diagnosed with bilateral pigment dispersion glaucoma by the glaucoma specialist and started on Latanoprost to both eyes noct., with a review in 6 weeks time. Patient declined private cataract surgery with iStents. The consultant confirmed that the patient was fine to proceed with cataract extraction without delay.
Following the appointment for glaucoma the patient asked me to refer her onwards to have bilateral cataract extraction with implants to correct her myopia. Again options were offered to go via the NHS hospital, or privately, or to an NHS funded private provider. One of the local private cataract providers offers NHS funded cataract extraction performed by a glaucoma specialist who also happens to work at the same NHS hospital as the glaucoma consultant that had diagnosed her glaucoma. She agreed that this may be a good option and consented to referral which was sent electronically to her GP surgery.
I now await her return for post operative refraction in the coming month or two.
Latest Articles



HCP Popup
Are you a healthcare or eye care professional?
The information contained on this website is provided exclusively for healthcare and eye care professionals and is not intended for patients.
Click ‘Yes’ below to confirm that you are a healthcare professional and agree to the terms of use.
If you select ‘No’, you will be redirected to scopeeyecare.com
This will close in 0 seconds